I saw a link on Reddit to a CDC presentation regarding additional vaccine doses for immunocompromised people (IP) (PDF). It outlines steps needed to have the CDC recommend additional doses, but we are still very far away from that. It appears that we are still in the reviewing data process, and still required FDA approval under the Emergency Use Authorization for the vaccines.
There were four slides under the section “What do we know now?”
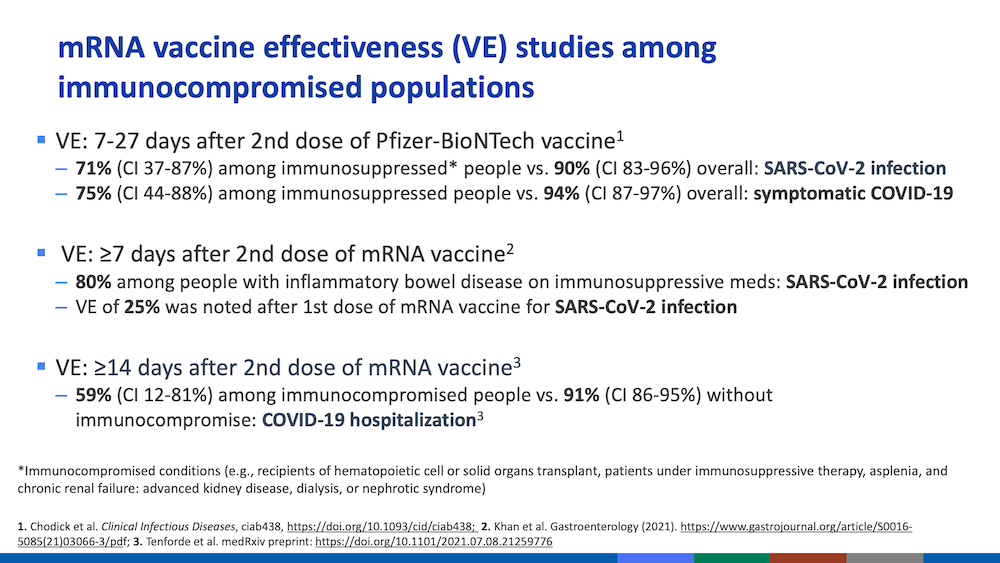
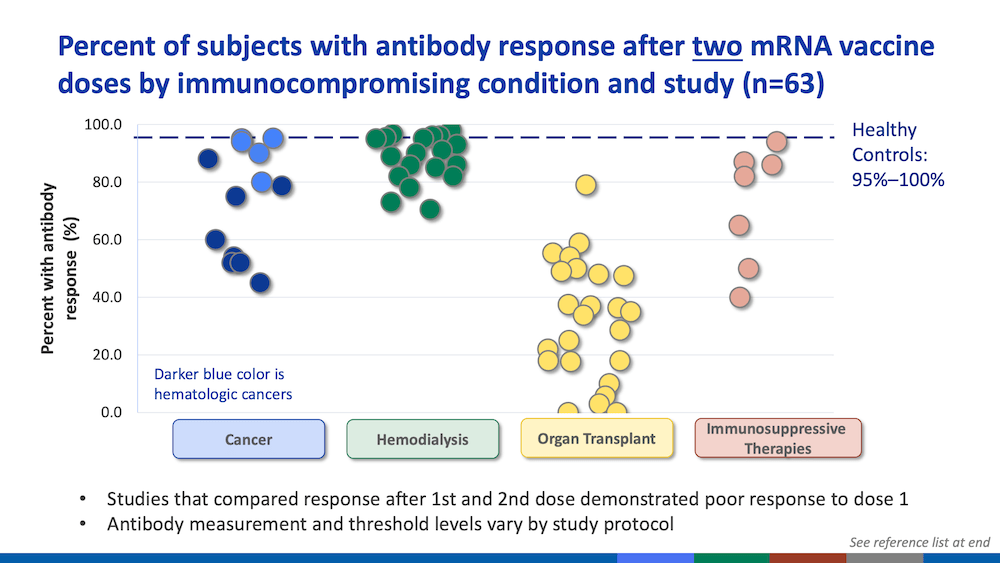
Again, since the data is not segregated by type of immunocompromised people, it is hard to estimate the increase in infection risk, even subjectively. My reading is that if there is a response to the vaccine, it is about 2/3 the effectiveness vs. non-IP. However, this may be lower for organ transplant recipients since the anti-rejection medications are specifically designed to mute any immune response.
In my case, I am slightly hopeful since my first vaccine shot was about 18 hours before surgery. I do not know if that is sufficient time for the immune system to develop any protection. Post-surgery, I was on a higher dosage of anti-rejection medications compared to today, but I do not know objectively whether it was a larger then normal dose. The transplant center did start to lower my dosage after about two weeks so there may be a slight chance that the second vaccine shot was somewhat effective, even though I did not experience any response side effects.
I am thinking about this daily because I am invited to my boss’s party next weekend. It is indoors but with a lot of open doors plus patios and balconies. In the past, the room was somewhat crowded. If I go, I am going to wear a KN95 mask, but it will be difficult to maintain a six foot separation from everyone else. It is difficult to manage risk where there is essentially no data. I am bringing my sister as my +1 guest. She is excited to go but she understands if I decide to skip the event.
