During dialysis today, a young boy along with two volunteers, came by to give me a gift for Valentine’s Day. I think he is a patient in the pediatric dialysis ward in the same building. The gift was a pencil with a note attached. It was a nice gesture; there’s not a lot of happiness at the dialysis clinic.
Last year, they handed out a Valentine’s Day gift too. It was a mini-donut with a note attached. The patient that came around was even younger, probably 4-5 years old, and he was in a wheelchair. I still have the note. <sad face>
It’s been almost two weeks since the surgery. I still keep a bandage over the incision even though it has stopped bleeding for a few days. I showed my arm to the nephrologist today during dialysis. He put his fingers on the bandage and gave a nod of approval. Evidently you can feel the blood rushing by in the newly connected vein. You can definitely hear the blood flowing; it makes a loud whooshing sound.
I don’t know how long it takes for the incision to heal. There is still sutures in the incision; I won’t get that removed until next week. Meanwhile, the area is still pretty swollen and looks pretty ugly.
My right forearm
I don’t know what the second small cut is for. I’m pretty sure the incision will eventually close up and heal but I’m a bit anxious about the actual fistula. I’ve seen many of them at the dialysis clinic and they are all really gross looking. I guess it depends on the age of the fistula but a lot of them are huge purple-ish bumps on the arm. An old Chinese lady was bleeding profusely from her arm after dialysis even though she sat and put pressure on the fistula for 15 minutes. Not looking forward to all this.
When I got to the dialysis clinic this morning, my pod or section was pretty empty. I think there were only three out of eight chairs occupied. Across from me was an older white lady with her son, and an Asian girl. I’ve seen both of them before with wheelchairs and scooters so I was surprised not seeing anything parked around their chairs. Dialysis really sucks already; not being mobile sucks even more. I was in a wheelchair for about two weeks after heart bypass surgery and didn’t enjoy being wheeled around.
Anyway, I was happy for a brief moment because I stupidly thought that maybe their condition has improved so they could walk in/out on their own. Nope. When the older lady was done, her son pulled a wheelchair from somewhere for her to sit in. A bit later, an older man (father?) and another girl (sister?) came in with an electric scooter to pick up the Asian girl. Bummer.
I mentioned before that there are lots of patients at the center using canes, walkers, wheelchairs, and scooters. I guess dialysis is usually not the only medical condition for kidney failure patients. Out of the five patients I can see in my pod now, one has a scooter, two are in wheelchairs, and the other two need a cane to get around.
The statistics on dialysis are grim. I post some numbers before but basically >50% of patients die by five years, and only a small percentage is eligible for a transplant. Why? If God is loving and we are His spiritual children, why is there so much suffering? This is only one disease. What about cancer patients? Mental illness? Life is so depressing.
==========
There is one dialysis patient, let’s call him H. He was in my pod the previous time I was on dialysis and now he’s in my pod again. H has one leg amputated below the knee so he is in a mobility scooter. He also requires medical transport, usually a minivan, to pick up and drop off at the dialysis clinic. I think H has a lot of other health issues. I used to sit right next to him and he is on the phone all the time with doctors, much like I am now post-heart surgery. I also heard a lot of complaints about H from the dialysis nurses. Evidently he’s been to almost every dialysis center nearby, and is a difficult patient. I know he complains about the needles in his fistula often, and would request a specific technician, even though that technician is working in another pod.
Anyway, it feels like H has been on dialysis for a long time. I took a closer look at him on the way out yesterday and he looked terrible, like his health had deteriorated a lot over the past few months. There was another patient at the clinic, let’s call him K, that has been on dialysis for over 25 years. I don’t know how H and K are handling dialysis. The only thing keeping me sane during dialysis sessions is the hope of a kidney transplant. I haven’t really thought about life on permanent dialysis. However, this is the norm for most dialysis patients; they are not qualified for a kidney transplant due to health, age, or other reasons.
DaVita’s website also has a page on Fluid Control while on dialysis. Since most dialysis patients don’t produce much urine, fluid control is very important in controlling blood pressure and avoid edema. Each dialysis session, the nurse listens to my lungs to see if there is any fluid in the lungs which could lead to shortness of breath or pneumonia.
The website also give a lot of tips on controlling fluid intake:
Limit the amount of sodium and spicy foods in your diet.
Be aware of hidden fluids in foods. Foods with high water content include gelatin, watermelon, soup, gravy and frozen treats like PopsiclesTM and ice cream.
Stay cool. Keeping cool will help reduce your thirst. Try drinking cold liquids instead of hot beverages.
Sip your beverages. Sipping will let you savor the liquid longer. Use small cups or glasses for your beverages.
Try ice. Many patients find that ice is more satisfying than liquids. Try freezing your allotted amount of water into an ice tray. You can also try freezing approved fruit juices in ice trays for a special treat. Remember to include the ice you consume when tracking your fluid intake.
Take your medicines with your meal, if possible. Try swallowing pills with applesauce instead of liquids.
Battle dry mouth by using mouthwash or brushing your teeth. Sucking on hard candy or a wedge of lemon or lime will also help.
If you have diabetes, maintain good blood glucose levels. High blood glucose levels will increase your thirst.
I pretty much do all of the above to control fluid intake, especially the ice trick. I carry a small thermos with me with ice chips. Rather than drinking water, I will melt a few ice pieces on my tongue and lips in order to quench thirst. It works fairly well.
I’ve been pretty good at keeping weight gains between dialysis sessions to minimum. I think I was averaging about 1.0 – 1.5 kg per two-day periods. After starting work though, I’ve been putting on more weight due to eating more during lunch, and drinking more fluids since the dispensers are very convenient.
Here’s a similar page from Fresenius’ website. They are the other large for-profit dialysis company, and they also make dialysis machines.
I created an account on DaVita’s website even though I’m not a patient. They have a lot of information on kidney failure, dialysis, and diet. I was specifically interested in their Diet Helper™ which has a lot of recipes and nutritional information.
Today, I received an email from DaVita pointing to the Employment page of their website. Basically, the email says dialysis patients should keep working if possible because it keeps you healthier and happier. My dialysis social worker says this too. It’s better for your mental health if you can continue working instead of quitting and getting Social Security disability.
Working and Dialysis
There could be another reason DaVita want their patients to keep working. 90% of their patients have Medicare as their primary insurance. Medicare reimbursement is pretty low so all their profit comes from the 10% with private insurance. I know I pay about 10x the Medicare rate to St. Joseph Hospital for dialysis in the past. Once I switch to Medicare as the primary insurance, that reimbursement amount will be a lot less.
Having not worked for three months and being on hemodialysis for most of that time, I would agree that working is good for your mental health. I was going crazy sitting at home all the time. Often I lost track of what day of the week it was since I didn’t have the weekly work schedule to keep track of time. Also a lot of my non-family relationships are with co-workers and not having regular contact for three months was very isolating. Of course, work has its own set of issues, namely stress and fatigue, but if you can work, you should try to work as long as possible.
I went to the KidneyDiseaseSupport Group at Saddleback Church today after dialysis. Since I didn’t switch shifts, I left the dialysis clinic at 1:10 pm and made it to the group at ~1:35 pm. The meeting started at 1:00 pm but I emailed the organizer so they know I will be late.
It was a full house again, with probably 35 people in attendance. I missed most of the introductions but there seemed to be several newbies who have no idea about ESRD, dialysis, and transplant. The organizer asked how I was doing so I gave a quick update about the PD catheter removal and fistula surgery to the group. Interestingly, in the group there was a donor who came with her recipient, and someone considering to donate a kidney to his mother. There was also another person who is on her fourth transplanted kidney in ~20 years. How is that possible when my wait time is 6-10 years?
Another gentleman also had fistula surgery last week but he had a new type of graft put in. He said his veins weren’t suitable for a regular fistula so they had to insert a graft. However, he was able to use the graft right away. I guess they can stick the dialysis needles directly into the graft, without waiting for the surrounding blood vessels to heal.
It was also interesting to see the large number of local patients that were listed for transplant at the Mayo Clinic in Phoenix, AZ. They even know which temporary housing to stay at while testing or recovering from transplant. I’ve considered this option but maybe I’ll give it more thought if both my living donors get rejected again.
When I started hemodialysis about 30 months ago, I noticed people bringing in lots of stuff: blankets, pillows, food, electronics, etc. Most people would have a bag to carry all their stuff. For the longest time, I resisted bringing a bag. Instead, I just carried everything by hand. Only on rare occasions would I bring my work backpack; that was usually when I needed to bring my work computer. I guess using a bag gives me a feeling of permanence, which I definitely did not want. After all, I was only on dialysis on a “temporary” basis while we figure out a living donor kidney transplant. Of course, that didn’t happen.
After returning to hemodialysis post-surgery, I was initially in a wheelchair because I did not have the strength to walk in on my own. Also since I sat at home all day, I was getting pressure sores on my butt and needed to bring in additional cushions. My mom gave me a huge bag to carry a seat cushion, a neck cushion, and a smaller bag with all my electronics (cell phones, iPad, headphones). I stopped using the huge bag when I didn’t need the additional seat cushion anymore. By then, my dad found a small messenger bag for all the other stuff I was bringing to dialysis. That bag was a bit too small, and he also wrote his Chinese name on it using permanent marker.
I finally went out and bought another messenger bag. I found some clearance items at Timbuk2‘s website and bought a “small” sized classic messenger bag. I wanted to get the extra small one but decided last second that I may want to put my old 13″ MacBook Air computer in the bag. It was ~$70 after tax. The bag is quite nice and feels quality-made. I’m still keeping my backpack for work since it has a lot more compartments but I can use the new back for dialysis, cardiac rehab, or day trips. At this point, I’ve accepted the possibility that I may be on dialysis forever, or until I die, so carrying a bag in doesn’t bother me anymore.
I’m still writing down blood pressure readings during dialysis, trying to figure out the pattern and how to minimize the fluctuation. Here are some readings from today:
Time
Systolic
Diastolic
Pulse
Notes
8:50 am
127
73
65
Standing
8:55 am
137
78
63
Sitting/legs up
9:07 am
148
83
63
Sitting/legs up
9:38 am
131
77
63
Sitting/legs up
11:08 am
178
88
65
Sitting/legs up
11:38 am
156
88
65
Sitting/legs down
12:45 pm
171
Sitting/legs down
1:00 pm
131
Standing
I can’t remember what I was doing between 9:30 am and 11:00 am but I missed several readings. My nephrologist agrees that likely the Metoprolol is being dialyzed out of my bloodstream during dialysis but she doesn’t want to prescribe more drugs yet. She did say the both the Metoprolol (beta blocker) and Olmesartan (ARB) are good for heart disease patients. NIFEdipine, even though it works great on me, doesn’t have any heart protection properties.
I handed a copy of my Medicare card to the front counter person. She said she will give it to my dialysis social worker. I hope they know how to coordinate billing since Medicare is supposed to pick up whatever my insurance does not pay. That is probably ~$3,000 since I am responsible for 85% of dialysis costs until I hit my out-of-pocket max. I still don’t know if Medicare covers my work insurance co-pays because I paid $280 already just for acupuncture co-pays.
Sitting in dialysis today, my left leg suddenly started hurting. To lessen pressure on my lower back, I usually sit upright in the dialysis chair. Most patients either have their legs up or sit fully reclined since that raises their blood pressure and lessens the chance of falling out of the chair. When I raised my legs near the end of the session, there was a shooting pain from the left heel up to the back of the knee. Since I get nerve pain occasionally from peripheral neurophy, it wasn’t anything to worry about at the time. The pain subsided a bit until I tried to get up and walk. Then the pain came back. Unlike my normal nerve pain that comes intermittently, this was pretty constant. However, I was able to limp along and it seemed to get better the more I walked.
Fast forward until now. The pain was present most of the day but worse when I straighten out my leg. I had two medical appointments this afternoon and when I got home, I tried to take a nap. I then noticed that the numbness in both legs is a lot worse. Since I have so many medical issues, I don’t know if this is from acupuncture, side effect of medication, more neuropathy, or deep vein thrombosis (DVT); the surface vein in my left leg was removed for heart bypass surgery.
Worse, my dad needed to go to the ER right about now. He hasn’t been able to urinate all day even though he feels like he needs to go. I volunteered to drive them to the ER but my mom won’t let me due to my leg pain. My sister was out of the house so they took an Uber to the ER. Wait… if I can’t drive to the ER, shouldn’t I go to the ER and have my leg checked out? If the pain numbness and pain doesn’t subside soon, I may need to go to the ER.
==========
It’s been about four hours since I posted the above and the pain in my leg is mostly gone. The more intense numbness is still there but that seemed to be the trend lately anyway. I took some regular Tylenol too so hopefully it’s not just the drugs masking the pain.
My dad is back from the ER. They had to insert a foley catheter to relieve the pressure. It was likely an enlarged prostate causing the issue.
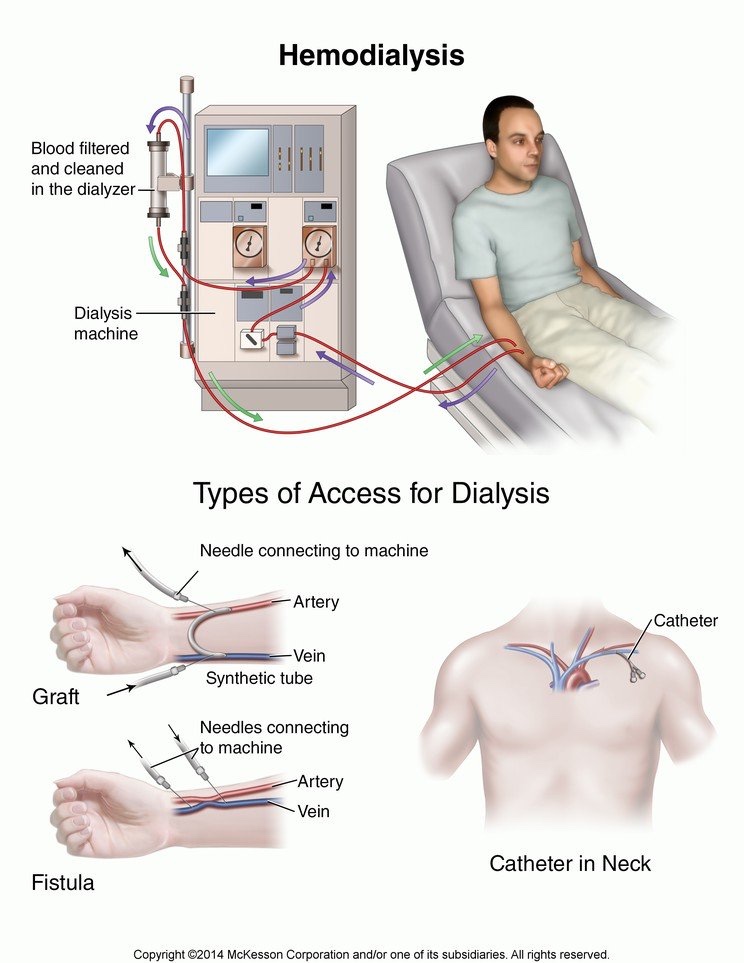
I use terms like hemodialysis and peritoneal dialysis often but most people probably don’t know what that means. I sure didn’t know anything about three years ago. I found some nice pictures online.
I go to the St. Joseph Hospital Renal Center three times a week for hemodialysis. It’s a non-profit dialysis center. Most patients are at a for-profit center like DaVita or Fresenius. Currently I have a catheter in my chest, my second one. I just had surgery to put in a fistula in my right arm above the wrist. When that matures and works, I’ll need to have the catheter removed, again.
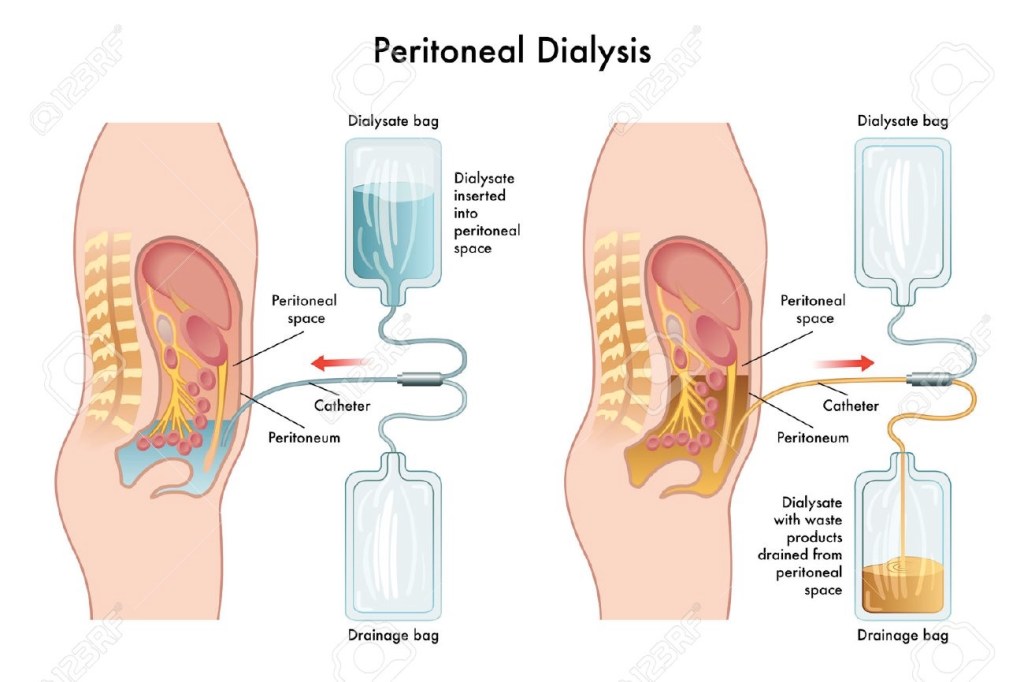
For six months I switched to peritoneal dialysis which required a different catheter. That was put in during April last year. Basically you put a dextrose solution in your abdominal cavity and let osmosis remove toxins and excess fluid by passing them through your abdominal wall membrane. The used solution is then drained and disposed. This fluid exchange can be done manually 4-6 times a day, taking about an hour each time.
Baxter home peritoneal dialysis machine
For me, instead of using manual exchanges, I has a machine that basically pumps fluid in and out of my abdomen overnight so I can work during the day with minimal interruptions. I would attach three bags of dextrose solution totaling 15 liters and the machine would cycle the fluid five times in and out of my abdomen. I also had to do a manual exchange around noon each day for extra dialysis. It turned out that my peritoneal membrane wasn’t suited for dialysis so I had to stop and go back to hemodialysis during the same time as my heart bypass surgery.
Home hemodialysis
Also available is home hemodialysis. Basically it’s a different machine that allows you to do dialysis at home. If my living donor kidney transplants don’t work out, that may be an option for me later.
We have a patient lift at the dialysis clinic. It’s new and quite fancy. It will weigh the patient while lifting them out of the wheelchair. There was an old one previously but they replaced it recently. The patient basically sit in a big canvas or cloth bag and the device lifts them from their wheelchair to the dialysis chair and vice versa.
Unfortunately, it gets a lot of use here. There are lots of wheelchair-bound patients who can’t transfer themselves to the dialysis chair. It just makes this place all the more depressing.
They finally renovated the lobby of my dialysis clinic. Their initial Medicare certification date appears to be 8/15/1977 so the center been around 40+ years, and the previous furniture in the lobby looks about that old. They also replaced the carpet with laminate wood flooring so it looks more clean and modern. For some reason, there are less chairs now so when the center is busy, there are not enough seats for all the patients waiting to be called.
Modern furniture and flooring
They also covered the walls inside the clinic with huge murals of scenery from tropical islands. The mural on my side of the clinic is a sunset scene so everything is very orange. You can see a bit of it on the left in the photo below. The wall used to be just beige.
While we’re fantasizingabouttravel, this seems to be the ultimate in fantasy travel. It’s only $160k per person, double-occupancy. You basically fly on a private Boeing 757 with only 50 seats, and all the attractions and accommodations are amazing.
$160k is a lot of money for 26 days. That comes out to ~$6k per day per person. Since the trip can take 48 guests, the total budget is $7.68 million. I could probably plan a great trip with that much money, though some things, like dinner at Kanazawa Castle may be hard to book for a nobody like me. I wonder how much profit margin they make on each trip.
Bombardier Challenger 850
There are also shorter trips on smaller private jets. It’s still not cheap; you’re looking at ~$35k for 14 days. This makes a lot of sense though. When I planned our Japan/Taiwan trip back in 2015, there was a lot of time allocated to traveling between destinations. It took us most of an entire day to get from Osaka to Taipei on Japan Airlines, and many hours to get from Tokyo Station to Shin-Osaka via the Tokaido Shinkasen. If we had chartered a private jet, then it would have been only a few hours.
This looks like an interesting itinerary. Five countries and only 5.5 hours of flight time between the different cities. You would spend four out of the 14 days transiting on a normal trip. I took a Trafalgar tour many years ago from London to Paris to Rome and we spent almost two days traveling between the cities by ferry and overnight train.
Of course none of this is possible without a kidney transplant. I don’t see a Dialysis in the Air option, though they probably could set up a hemodialysis machine inside a wide-body jet. The patient would have to do dialysis on the jet, probably while parked at an airport, but it will cost a lot for a dedicated nurse and space on the plane for the dialysis machine. Maybe it’s more feasible for peritoneal dialysis patients since all you need is someone to coordinate moving cyclers and supplies to hotel rooms from the private jet. It will be up to the patient to run their nightly dialysis program.
==========
OK, they are ridiculously expensive. I looked at one of their Tailor Made custom tours of Nice and Monaco. For four days, it’s ~$5k double occupancy, so about ~$10k for two people. The hotel listed in the itinerary, Hôtel La Pérouse, is only $210/night in May for an Economy room; even if you book a Deluxe room, it’s ~$750/night, breakfast included. If you go to all the places listed in the trip itinerary, the total cost of admissions is <€60. Other than the hotel breakfasts, there are no other meals included. Add local transportation, airport transfers, and the cost for a private guide for a few days, it’s still way less than $10k. I guess there’s some value in coming up with the itinerary. A friend planned her Europe trip by copying itineraries from Rick Steve’s website, or you can just use a travel agent.
I drove to dialysis today by myself even though I was supposed to wait 24 hours. I was going to ask my dad to drive me but by the time I remembered, I was already on the road.
I showed my dialysis nurse the bandage on my right arm and told them I had the surgery done. A couple of nurses came by to take a look and they were more excited about the surgery than I was. I think they really don’t like using the chest catheter unless it’s absolutely necessary. One of the supervising nurses pulled out her stethoscope, listened to the surgery site, and gave me a thumbs up. Not sure what she was listening for but I’m glad it was good.
$197!
They continue to challenge my weight at dialysis. Even though my dry or ideal weight is 92.0 kg, they try to take more fluid out since they want to avoid edema or having fluid build up in the lungs. I left dialysis at 90.9 kg; that’s probably my lowest ending weight in over two years of hemodialysis.
I fell asleep early last night and woke up at around 3:30 am this morning. I thought I didn’t take my 30 mg of NIFEdipine ER before sleeping so I took another one. I then took all my regular medications this morning, including the 10 mg of NIFEdipine.
When I got to the dialysis clinic and measured my standing blood pressure, it was 90/60. Either I doubled up on the ER pill, or took it too late so it’s adding to the three medications I took this morning. That’s one issue with having too many meds. You lose track of which ones you took when sometimes.
The first blood pressure reading sitting down was 120/69 which is still a bit too low. It should increase when the Metoprolol starts gettingdialyzed out by the machine.
==========
Ha! The machine too another blood pressure reading while I was clicking “post” on this post. It first came back as 78/50. I told the nurse that can’t be right so she tested again and it came back at 110/64. Better, but I definitely messed up my medication schedule this morning.
==========
Time
Systolic
Diastolic
Pulse
Notes
8:45 am
90
60
—
Standing
8:46 am
102
—
—
Standing
8:53 am
120
69
59
Sitting/legs up
9:23 am
110
64
63
Sitting/legs up
9:58 am
134
71
59
Sitting/legs up
10:28 am
139
82
59
Sitting/legs down
10:58 am
139
82
60
Sitting/legs down
11:28 am
145
87
59
Sitting/legs down
11:58 am
158
95
60
Sitting/legs down
12:28 pm
163
93
58
Sitting/legs up
12:58 pm
178
—
—
Sitting/legs up
1:03 pm
138
—
—
Standing
So the systolic numbers goes really high right at the end. I’m thinking the 178 reading is wrong since it then drops by 40 points on the last standing measurement. With such huge variations in blood pressure readings over four hours, it’s all dependent on the level of medications in my bloodstream. I feel like I’m cheating each time I take the extra 10 mg of NIFEdipine since it’s like an emergency drug: works quickly and wears off fast. I measured my blood pressure yesterday around 2:00 pm and it was 192/100. All the morning meds probably wore off by then. I don’t think it’s good for my body to have blood pressure fluctuate like that.
I check the dialysis blood pressure measurements from the past few sessions and the drop in blood pressure for the last standing measurement is pretty large. That just makes prescribing medication that much harder since they can’t lower my sitting blood pressure too much in case I stand up and pass out.
There are four “pods” at my dialysis clinic and each is staffed by a nurse and one or two technicians. I used to be in C pod previously but now I’m in B pod after switching shifts. They rotate the staff around so if you stay here long enough, everybody gets to work on you. I think the technicians rotate every three months and nurses rotate every six months.
Today is the first nurse rotation since I came back to this dialysis clinic. In total, there are four regular nurses and two supervisors that fill in when it’s busy, or if someone is out. Most are Filipino with one Hispanic and one Korean nurse. I know all of them pretty well because only the nurses can connect me to the machine because I have a chest catheter instead of a fistula.
One of the nurses said that six months is too short since you get to know your patients better over time. I have to explain to the “new” nurse my blood pressure history and why I’m on three medications since it’s all new to her.
I’ve been so focused on researching transplant centers that I didn’t realize Medicare rates dialysis facilities. I searched for my dialysis clinic, St. Joseph Hospital Renal Center, and they only have a 4/5 star rating for quality of patient care, but a 5/5 for patient survey. Looking at the rating details, I think they got dinged for a lower % of adult patients who had enough waste removed from their blood during hemodialysis. That explains why they want me to increase my dialysis time when my Kt/V result came back at 1.18 (should be at least 1.2). Across the street from my dialysis clinic is Satellite Healthcare Orange, which was my center for peritoneal dialysis. They have 5/5 stars for both ratings; maybe I should have gone there for hemodialysis instead of returning to St. Joseph. There is also a DaVita facility nearby. They have a 5/5 from Medicare but only 3/5 from their patients.
Some other interesting statistics:
DaVita
St. Joseph
Satellite
California
National
Preventing bloodstream infections
As Expected
As Expected
Better than Expected
Adult patients who had enough waste removed from their blood during hemodialysis
96%
89%
97%
96%
97%
Adult patients who had enough waste removed from their blood during peritoneal dialysis
97%
N/A
93%
89%
91%
Rate of fistula
Better than Expected
As Expected
As Expected
Adult patients who had a catheter (tube) left in a vein for at least 3 consecutive complete months for their regular hemodialysis treatments
As I was debating the fistula surgery, I noticed most of the patients at St. Joseph is getting dialysis through a fistula. From the data above, there’s more catheters at St. Joseph than at DaVita and Satellite. Medicare states that higher rate of fistula is better, and lower usage of catheter is also better. This also likely affected St. Joseph’s Medicare rating. Sorry!
For patient survey, DaVita got average ratings for kidney doctors and clinic staff, while St. Joseph and Satellite got better than average numbers.
Crap! Just what I need in my life right now… more time on the dialysis machine. My nephrologist came by today during dialysis and told me my last Kt/V result was 1.18 even though my URR was 65%. Minimum clearance for hemodialysis is 1.2. She was fine with the number but the dialysis clinic is unhappy. I think they are regulated very closely by the state department of health, and it looks bad if a patient is not getting adequate dialysis.
Since I’m still using a chest catheter, the maximum flow rate is 350 mL/min and I’m maxed out. A mature fistula can work at 600+ mL/min so more blood flows through the machine and filter. Starting next session, we’re adding 15 minutes each day to my dialysis time. It sucks but I guess it’s better than adding 30 minutes.
Incidentally, about 7% of body weight is blood so at 92.0 kg, I have about 6.5 liters of blood. At 350 mL/min for 3.5 hours, that means the machine can filter 73.5 liters of blood or 11.4 times my blood volume. That filter is not very good. In comparison, for a 70 kg male adult, blood flow through the kidneys is 1.2 – 1.3 liters per minute
It’s been about a week since I last flushed the PD catheter so I quickly flushed it tonight with 1.5% dextrose solution. I didn’t leave the solution inside at all so there was probably no UF. The solution bag had 2,500 mL of fluid so I did two flushes of ~1,250 mL each. The initial drain had a bit of blood in it so the drained fluid had a slight pink tinge but nothing like the craziness from January 1st.
Since the surgery to remove the PD catheter is this Friday, today’s flush will likely be my last. By next week, the catheter will be gone and I can start tossing all the remaining supplies. The PD catheter was put in on April 11th last year so it’s been almost 10 months. I kind of got used to having huge quantities of dialysate solution in my hallway and study so it will be weird to get all that floor-space back. In hindsight, I should have just gotten a fistula instead of the PD catheter. I was pretty much getting no dialysis during the last couple months of PD so who knows what additional damage I did to my body. Most likely I lost the last bit of residual kidney function, which makes hemodialysis and fluid control much harder this time around. I also fell asleep driving quite often. Luckily AutoPilot kept the car from crashing but I don’t want to try that again.
The medications continue to work. I took all three at around 8:15 am this morning before dialysis. Here are the first several readings:
Time
Systolic
Diastolic
Pulse
Notes
9:02 am
117
74
64
Standing
9:13 am
135
75
63
Sitting/legs up
9:43 am
141
79
60
Sitting/legs up
10:13 am
151
83
60
Sitting/legs up
10:43 am
145
86
60
Sitting/legs down
I only have two data points since I started taking all three medications before dialysis, but if you look at the numbers from last session, my blood pressure increased at the 10:18 am reading. Likewise, there seems to be an increase today at 10:13 am. One or more medication is getting dialyzed out about an hour into dialysis. My guess is the Metoprolol. There was a study done on Olmesartan and it appears resistant to dialysis.
==========
Blood pressure increased to 168/96 at 11:43 am. Either something else is getting dialyzed out or the 10 mg of NIFEdipine is wearing off since it’s such a low dose.
==========
Remaining readings continued from table above:
Time
Systolic
Diastolic
Pulse
Notes
11:13 am
148
90
60
Sitting/legs down
11:43 am
168
96
62
Sitting/legs down
12:13 pm
156
88
60
Lying down
12:43 pm
157
89
62
Lying down
12:50 pm
159
92
62
Sitting/legs down
12:52 pm
127
74
65
Standing
I’m surprised that both number dropped so much on the final standing measurement. The initial increase at the beginning of dialysis when I sat down wasn’t that large. That means I still have orthostatic hypotension.