The US Senate passed a bill yesterday to provide immunosuppressive drugs post-transplant for life. Previously, Medicare only pays for three years of medication post-transcript. For patients that won’t qualify for Medicare after that date, they have to find their own insurance or risk losing their transplanted kidney. I read that about 375 patients die each year from losing Medicare and not being able to afford the needed medication. This is supposed to save $400M over 10 years since thousands of patients can avoid a return to dialysis, which is also paid for by Medicare.
For me personally, this means I can consider retiring post-transplant. I’m in my early 50’s so if I go through the transplant soon, I will run out of Medicare coverage in my mid-50’s and need to find insurance coverage for 10+ years. That typically means getting a job and work-provided insurance. I do need to find out if Medicare will only pay for immunosuppressive drugs or will they continue as my primary health insurance, paying for 80% of all claims.
So I guess I was wrong about the timeline. It seems like we’re a few weeks away from a FDA approved vaccine from Pfizer. The question is who will get the first few doses available. From STAT news:
Separately, STAT has learned that senior leaders in the Trump administration’s coronavirus response are pressing for adults 65 years old and older to be given first access to the vaccine. That approach contradicts the position of a committee that advises the Centers for Disease Control and Prevention on vaccine policy; the Advisory Committee on Immunization Practices has signaled for months that it will recommend health care providers be at the front of the vaccination line.
I think frontline healthcare workers should be one of the first to get the vaccine since their exposure risk is very high. It would also be a good environment to test the effectiveness of the vaccine in the wild. Nursing home patients make sense as well since their has been so many deaths in that population. I think the Trump administration is focused on seniors over 65 because they are higher risk, but also majority Republican voters as well. You can target the seniors in the nursing homes but if the rest of the seniors are socially distancing or isolating themselves, a few more weeks/months seems like low risk versus not vaccinating healthcare workers.
Since I have lots of health risks, I’m probably in the front of somebody’s list. Although it would be nice to get the vaccine and live vicariously, I think I can wait a few months since I’m working from home anyway, and the kidney transplant may be soon. Maybe I’ll get the vaccine post-transplant due to all the immunosuppressive drugs I have to take.
Speaking of echocardiograms, my cardiologist just posted her notes on the repeat exam to the online patient portal. Again, there were a lot of words and numbers that don’t mean anything to me, but I did see a few important results.
LV ejection fraction is normal, at 57.1 %.
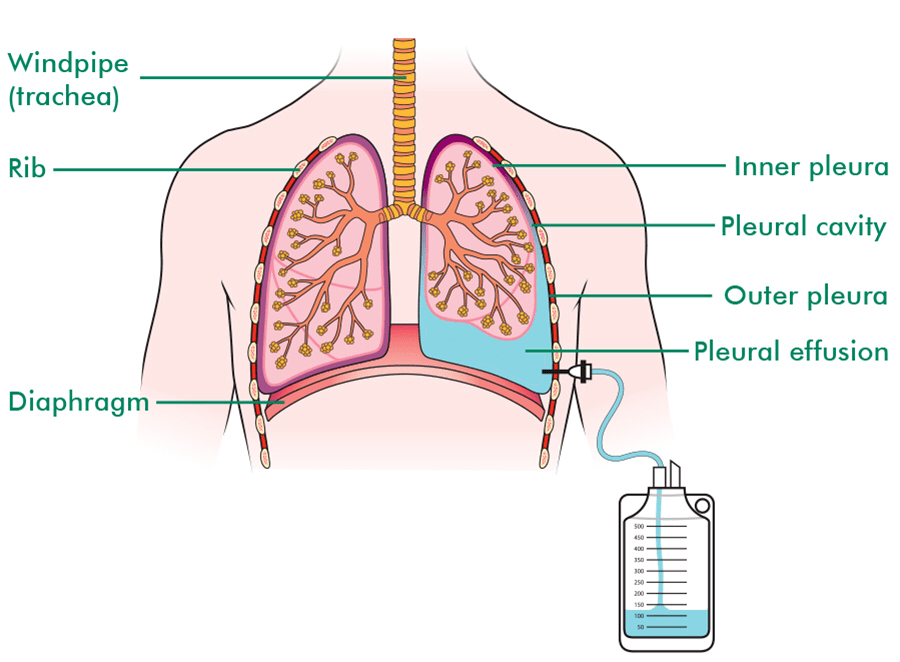
Prior examinations are available and were reviewed for comparison purposes. Compared to the study dated 10/29/2020 there is no longer presence of pleural effusion.
The last echo exam already came back with a LV ejection fraction of ~51% so this test just confirmed the normal results. The most important results is the “no longer presence of pleural effusion.” When the cardiologist told me I had fluid in my lungs, I guess they were telling me I had pleural effusion. It is defined as:
A pleural effusion is excess fluid that accumulates in the pleural cavity, the fluid-filled space that surrounds the lungs. Excess fluid can impair breathing by limiting the expansion of the lungs.
That’s exactly what happened to me suddenly back in April and lasted for about six months. Initially, we thought it was a symptom of my a-fib condition, and it did improved a bit after the ablation procedure. However, I was still having issues breathing, and a later chest CT scan showed there was still fluid restricting my breathing. With the recent “more aggressive” dialysis, I think we were finally able to remove most, if not all, the excess fluid so I won’t need to physically drain the fluid by other means.
I hope the results were sent to UCLA and they’re satisfied with the updated results. That leaves the colonoscopy as the final hurdle for my kidney transplant. Yay!
==========
Now that I know what I’m looking for, I found this in the results from the first echo exam:
Incidental Finding: There is a moderate pleural effusion noted in the left lateral region.
Interesting that my cardiologist noted it as an incidental finding, yet it was enough for UCLA to halt the transplant process until the fluid was removed and I was retested. Another peril of having two teams of specialists reviewing your medical results. 😷
I am scheduled for another echocardiogram this morning. UCLA Transplant Center requested it after my previous one since there appeared to be fluid in my lungs. After running the Crit-Line monitor during dialysis for the past two weeks, I think we took out a lot of excess fluid so hopefully UCLA will be satisfied with the results.
==========
It’s 11:00 am and I’m back home. The echo scan tool about 20 minutes. This time, I was looking at the machine and saw most of the scan results. Since it’s an ultrasound, the pictures were blurry but you can see the heart muscles and valves pretty clearly. The tech had to freeze frame and trace out several heart cavities on the screen; I guess that’s how they determine volumes. It was pretty weird looking a moving images of your own heart. The worst part of the exam was that the room was pretty cold and you have to remove your shirt. I was shivering for the first few minutes until he covered me with a small towel. I can’t interpret anything from the screen so I have to wait for my cardiologist to call me back.
I really like my cardiologist. She called me again today in response to a message I sent her late last week. Instead of writing a reply, she decided to call instead. I had asked her about the “aggressive” dialysis comment from the UCLA transplant cardiologist and she said the echocardiogram showed I still have fluid in my lungs. She recommended that I stop taking my hypertension medication before dialysis so there is more “room” for the blood pressure to drop as the machine removes excess fluid. I told her that the dialysis center was already removing more fluid, and last two sessions showed a drop in blood pressure instead of the typical increase. Anyways, she ordered another echocardiogram to be done in about two week. Hopefully I will be rid of the pulmonary edema and UCLA will be satisfied with the health of my heart.
I just received a call from my transplant coordinator. After their cardiologist reviewed my most recent echocardiogram, they want me to do another one after some “aggressive” dialysis. I believe the reason was that the last test showed high blood pressure and they want me to try again after some fluid removal. This matches what the Crit-Line thingy showed today, and they dialysis center is already trying to remove more fluid.
However, the instructions seem kind of vague. WTF is more “aggressive” dialysis? You can’t really change the cleaning cycle so I guess we’re all talking about more ultrafiltration or fluid removal. I sent a message to the transplant cardiologist, my local cardiologist, and also my nephrologist asking them what to do. Since this is yet another hurdle on the way to getting a kidney transplant, I want to make sure I’m not being rejected due to some random test result.
I just had a video call with my transplant social worker from UCLA. It’s another hurdle in the long path to a transplant. It’s actually the third time I’ve spoken to a social worker from UCLA; each time there’s a potential transplant surgery, I have to go through the entire process. The questions were pretty generic and I don’t think there were any problems or red flags. The only item that came up was having a backup caretaker post-surgery since my mom doesn’t like freeway driving. I spoke to my friend who was a potential live donor and he volunteered to help out. I gave his contact info to the social worker so I think that part is done. I just have to wait a month for the colonoscopy appointment.
I had an echocardiogram done this afternoon, at the request of my cardiologist and UCLA Transplant Center’s cardiologist. The procedure is basically a heart ultrasound and it only took 15 minutes. Weird that such a short test can affect the rest of my life.
The tech had me take off my shirt and lie down on an examination bed. Most of the test was done lying on my left, which is not that great for me. Even almost a year after the bypass surgery, I still feel pressure when I lie down on my left. I think I mentioned in a previous post that my cardiologist wanted to double check the LV EF (ejection fraction) number since my latest results from the Lexiscan was pretty low. She said the Lexiscan EF results were not as accurate as an echocardiogram; let’s hope that’s true and the results are better this time.
During dialysis, I got a phone call from my cardiologist’s office. I had asked them to send in the results of my Lexiscan heart stress test to UCLA Transplant Center. UCLA’s cardiologist (I’ve seen him before in April) then requested an echocardiogram (echo). My transplant coordinator at UCLA also called me a bit later about the same issue so I told her the echo was already scheduled. I guess things can move fast when they want to. My echo test is this coming Thursday at 1:45 pm.
I’m not sure how to feel about this. This one test has been a mini-emotional rollercoaster. Initially UCLA said I didn’t need a heart stress test since I had bypass surgery. This was confirmed by my April appointment with UCLA’s cardiologist. After a phone meeting with the transplant center director, they now say they want a stress test. I was still okay since I passed the same test in 2016 with a “bad” heart. After the results came out, I wasn’t so sure since my LV EF was <40%. For a few weeks, I was sure that would rule me out for a transplant for life. Then my doctor friend said that number wasn’t too bad, and I could probably raise it through exercise. Good thing I just got a deep cut in my foot. My cardiologist then called to explain the test results and her comment that she didn’t see anything that would prevent a transplant made me feel optimistic again. Next, I find out that UCLA never received the test results so I asked my cardiologist office to send them again. Now I feel conflicted since it’s good that I wasn’t rejected based on the heart stress results, but the fact that they want another test worries me again.
Now multiply this by 100 and you can get a sense of my feelings and emotions over the past 4-5 years as I found out about my ESRD condition and starting dialysis.
I had a phone call with my cardiologist today. I thought it was supposed to be a Zoom call but we just talked on the phone. She was very cheerful; I guess that’s a good trait for a cardiologist since her patients all have some heart issues.
She explained the results of the Lexiscan test to me. Basically they were looking for defects or damage to my heart, and also to see if it is reversible. The results showed that I do have some heart tissue damage (infarction), but it’s not reversible. I probably suffered one or more heart attacks prior to the bypass surgery. That was corroborated by my high troponin test results days prior to the surgery showing heart muscle damage. However, she also said that there’s nothing in the test that would rule me out for a kidney transplant. There is some elevated risk, but since I did not have a stroke before, and the bypass surgery basically “rebuilt” my heart, I should be fine for transplant. Of course, the final decision is up to the surgical team at UCLA, but she will send her findings in to them. She also said the chest CT scan indicated I had probably up to 500 mL of fluids in my right lung, but dialysis should be able to take care of that. I think we’ve taken care of that already since my breathing is near normal as my nephrologist dropped my dry weight to 80.0 kg. Finally, she was agreeable for me to stop taking my blood thinner a week prior to the transplant surgery without the need to switch to coumadin/Warfarin. Yay for small victories!
Finally, I made the initial consultation to see a doctor about colon cancer screening. That is (hopefully) the last test I need to take to be cleared for transplant. My sister is already cleared as a donor so I’m finally hopeful that a live donor kidney transplant may actually happen.
I received a call yesterday from the UCLA Kidney Transplant Center. For some reason, the caller ID said “Anonymous” but I didn’t see the call either. Anyway, they wanted to verify my email address and send me a Financial survey form. I filled one of these out several years ago. I am already on Medicare which pays for either all of the transplant fees or only 80%. Maybe they want to be sure that I can pay the 20%? I have work insurance through Blue Shield that should pick up any charges not paid by Medicare.
UCLA also wanted me to call Blue Shield to update my coordination of benefits file. This was the huge mess-up from earlier this year where Blue Shield had the wrong cut-over date and thought it was secondary payer when they were supposed to be primary. I thought this was already taken care of but I called to check just in case. Maybe when UCLA calls me back they can clarify.
==========
Update: 10/21/2020 10:00 am
So UCLA didn’t call me back but the person that called did send me a form via email. The form was a sign-able PDF. It asked for my monthly salary (including stock awards?) and checking/savings account balances. When I completed the form, I digitally signed it and sent the form back to UCLA. Today, I got another email that said they could not accept digital signatures and I had to sign the form with a pen… old school style. Not a problem, but why did they send me a digital signature form if they can’t accept it? Fortunately, they do accept a scanned PDF form. I thought I had to find a stamp and envelope to mail the actual paper form.
Dialysis went well today. The fistula worked fine and didn’t give me any flow issues or pain. However, they had to go with the new insertion point again. The tech said the original arterial needle insertion point has scabbed over too many times and turned hard, so we may not be able to use that site again. I now see why people have fistulas that becomes unusable over time and have several fistula operations.
I didn’t get much sleep last night again so I played games for about an hour then slept until 9:15 am. This is the best kind of dialysis session, where I’m asleep for most of it. Since today is Saturday, there wasn’t a nephrologist doing rounds and waking up patients. Once again, I left the clinic at an all-time low weight of 81.1 kg. That’s about 179 pounds. I haven’t been under 180 pounds since high school probably.
I’m kind of stressed out about my heart stress test. The results look bad based on the LV EF number. I think part of me is already assuming that I will be disqualified from transplant surgery and the 3x/week dialysis sessions are going to be a permanent part of my life.
Nobody has called me yet but the written report is online on St. Joseph’s patient portal. I read it but don’t really understand anything that was written. I had to look up a lot of words but I still don’t know what the results are. I guess it’s up to UCLA to decide whether my heart is healthy enough for a transplant. I’m hoping one of the St. Joseph cardiologists or UCLA will call me with more info.
IMPRESSIONS:
Moderate LV enlargement with moderate post-stress LV systolic dysfunction (post-stress gated SPECT LV EF 37%).
Medium to large sized fixed inferior and inferolateral defect consistent with infarction.
Compared to the report of the study dated 11/16/2016, the inferior and inferolateral infarct complicated by moderate LV systolic dysfunction are new.
I guess LV stands for left ventricle, and the dictionary defines infarction as obstruction of the blood supply to an organ or region of tissue, typically by a thrombus or embolus, causing local death of the tissue. I think the event is what caused me to go to the ER and having to get the bypass surgery. I did meet with a cardiologist from UCLA back in April who review my files from St. Joseph and he cleared me for transplant.
There are so many tests and decision points in this whole process. I feel like my sister or me can be rejected at any point for one of a thousand reasons. I wonder how any live donor transplants are performed? The donor and patient must be super healthy.
==========
Crap. From this website that explains EF (ejection fraction), under 40% indicates heart failure or cardiomyopathy. My result is 37%, which means the left ventricle is only pumping out 37% of the blood during each contraction. I hope this doesn’t have anything to do with my current fluid overload problems. Now I’m stressed out and worried that I will be ruled out for the transplant.
I’m also angry with UCLA for delaying the transplant for so long. One of my fears initially is that when UCLA was finally ready for transplant, my health had deteriorated over time so I don’t qualify for a transplant anymore; over 90% of dialysis patients cannot get a transplant. Now it looks like this worst case scenario may be coming true.
I guess I can post about this since there was no follow-up. About six weeks ago, I got a chat message on Reddit from a reporter with Pro Publica. She saw some of my posts/comments on Reddit about how long it has taken to try and get a live donor transplant. I believe she was planning on writing a story on the subjective hurdles of getting a kidney transplant. I replied agreeing that I would speak to her if she kept it anonymous since at the time, I was still waiting for UCLA Transplant Center to approve my sister as a donor. She replied that she would keep my name off the story and asked for times to contact me. I replied again with my availability, then nothing. I checked Pro Publica for her stories and she has not published anything about kidney transplants yet. Maybe the story was cancelled or delayed?
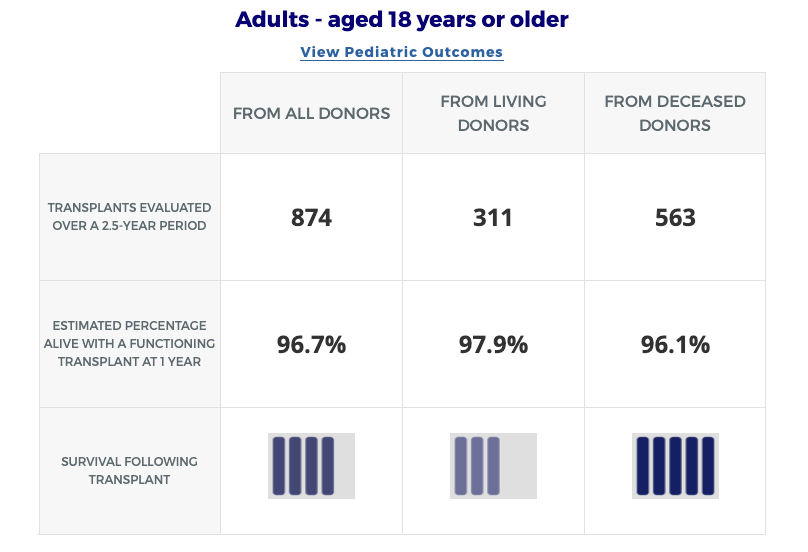
Regardless, I think we need to shed more light on this topic. The National Kidney Foundation has some depressing statistics on kidney failure. They claim that there are 2 million people on dialysis worldwide and that only represents 10% of the population that needs it. Outside of rich countries, most kidney failure patients just die. The transplant centers should be doing more transplants, not less. I’ve always felt they are trying to preserve their post-surgery scores rather than helping as many people as possible. I guess it’s hard to avoid since SRTR publishes reports like this all the time.
On the latest report, it says UCLA has a post-surgery survival rate of 97.9% for living donor kidney transplants. That’s pretty good but useless to me if they won’t do the transplant. I would still risk it if the number was as low as 80% since dialysis really sucks. My nephrologist said they were pretty risk adverse on transplant candidate selection. It’s a research hospital… shouldn’t they be taking more risks?
Anyway, I hope the Pro Publica story gets written and published, whether or not they include my experience. It seems like the health agencies could do more to inform people about living donor transplants and encourage new developments in kidney care and dialysis treatments. Here is a Nature paper on the state of dialysis and it’s pretty sad.
Abstract
The development of dialysis by early pioneers such as Willem Kolff and Belding Scribner set in motion several dramatic changes in the epidemiology, economics and ethical frameworks for the treatment of kidney failure. However, despite a rapid expansion in the provision of dialysis — particularly haemodialysis and most notably in high-income countries (HICs) — the rate of true patient-centred innovation has slowed. Current trends are particularly concerning from a global perspective: current costs are not sustainable, even for HICs, and globally, most people who develop kidney failure forego treatment, resulting in millions of deaths every year. Thus, there is an urgent need to develop new approaches and dialysis modalities that are cost-effective, accessible and offer improved patient outcomes. Nephrology researchers are increasingly engaging with patients to determine their priorities for meaningful outcomes that should be used to measure progress. The overarching message from this engagement is that while patients value longevity, reducing symptom burden and achieving maximal functional and social rehabilitation are prioritized more highly. In response, patients, payors, regulators and health-care systems are increasingly demanding improved value, which can only come about through true patient-centred innovation that supports high-quality, high-value care. Substantial efforts are now underway to support requisite transformative changes. These efforts need to be catalysed, promoted and fostered through international collaboration and harmonization.
I rushed home from dialysis today to watch a live NKF (National Kidney Foundation) webcast regarding kidney transplants. The program was supposed to be about what to expect during the first 100 days of a transplant. The webcast had three speakers: the NKF host, a transplant doctor, and a transplant patient. The patient received a deceased donor kidney about six month ago.
Like most kidney disease presentations, this was pretty basic. Or maybe I’ve read/heard all about it for the past four years. I don’t think I learned that much from attending except that the deceased wait list is not absolute. They do some line skipping if there is a particularly good match or some type of antigen criteria. Once again, I’m surprised at the lack of knowledge regarding kidney disease. Of course no one knows anything initially, but if you are diagnosed with this lifelong chronic condition, wouldn’t you do some research? It seems that new patients don’t even do the most basic Google search for more info.
There are two more webcasts in the series. Hopefully they are more informative for those already on dialysis and the transplant list.
==========
My dad was watching the webcast with me and asked me about having a packed bag ready in case I get a call. I think they meant if you’re near the top of the list in your area but not #1, you may get the next kidney depending on a few different criteria. There are over 2,000 people waiting for a kidney transplant at UCLA, and they’re one of a dozen transplant centers in Southern California that share the same list. I’m probably another 5-6 years from the top of the list. I don’t think I need to pack my bags yet.
I’m not sure what to post here. Since it’s #777, it seems special but I feel like I haven’t had any luck or breaks during the past five years. Scratch that, maybe no luck going back 14 years to the divorce. Some Christians think divorce is a huge sin, while others say it’s just another event in your life. I did feel for a long time that having gone through a divorce was like a scarlet letter on your chest, and indicative of somehow losing God’s blessing.
First few years after divorce was full of depression and loneliness as my sister had moved to Portland and my parents moved to Canada. I was pretty much alone for a couple of years, just working and sleeping. Then I spent a few years traveling to China with my friend to help out his factory with planning and fundraising. It sounded fun but I still was lost and didn’t know what to do next. Then parents moved back to California and we bought a house together, and I switch jobs after 12 years at the same company. Soon after, I found the church I’m attending now then the kidney problems started. From declining kidney function, to signing up for transplant, to dialysis, to today. It seems to be one health calamity after another: kidney failure, dialysis, donor rejections, peritoneal dialysis failure, heart bypass surgery, atrial fibrillation, and now tons of dental work.
My greatest fear right now is that this string of bad luck or whatever you want to call it will continue. I need my sister to pass her health tests later this month, and I need to get past my heart stress test and colonoscopy. Any of those could derail the transplant train for good.
SRTR has new reports out on all the transplant centers. It appears that they update their data every six months. Here is the page on UCLA’s kidney transplant program. I blogged about this way back in mid-January. The updated reports have six months of additional data.
I was mainly focused on looking at wait times for patients with blood type B, and comparing that to other centers across the country. Six months ago, it seemed California had very long wait periods, and it was worse than average for blood type B patients. Well, nothing has changed in six months. If anything, the statistics got a bit worse. In the prior report, it said about 20.2% of blood type B patients received a transplant after 3-years. Now the number is 19.5%. It’s slightly worse but I don’t know if it’s statistically significant. In comparison, the national number for all patients is 26.6%, up from 25.4% six months ago. So, the entire country got slightly better, while blood type B patients at UCLA got slightly worse.
The 63-page report can be found at the SRTR website, as well as prior reports.
On the video call last Friday, my new transplant coordinator said that she would put documents on the myChart portal for me. Unlike the St. Joseph Hospital portal, I don’t think I got an email notification. I just check now and there are several documents and a list of things for me to do.
Nuclear medicine stress test (Lexixcan)
Transition off my current blood thinner medication
Check with primary physician if I need a colonoscopy
Unfortunately, I already had a referral for a colonoscopy from my primary care doctor. Before I was able to follow-up, the heart surgery hit and then COVID-19 and here we are. I’ve already scheduled my CT scan for the thoracic surgeon for next week. Coincidentally, the cardiology department at St. Joseph called me today to schedule the Lexiscan. The person on the phone said my cardiologist ordered it for my transplant. UCLA must have called her office since I didn’t update any of my doctors on the transplant progress yet. I hope the two tests are not related, i.e., the stress test will show my heart is okay (should be post-surgery) even though something in the chest cavity causing pressure in my chest.
==========
Also, my transplant coordinator called me Monday to tell me that the medical director we spoke to last Friday may call me to talk to me again, since we didn’t discuss the minimal cancer risk. I told her I was available in the afternoon, and he hasn’t called yet. He did call my sister however, to let her know that they are progressing with the transplant. Weird.
We had our call with UCLA transplant center‘s medical director this morning. They wanted me to log on 30 minutes before the meeting so I was at my sister’s house at 7:00 am this morning. The call used some meeting function in myChart from Epic, which is a large provider of online health data according to my sister. The issue is only I had an account at UCLA Health and they wanted both of us on the call.
A coordinator came on 20 minutes before the meeting and got my medication list updated, then we spoke to the doctor for about 20 minutes. He didn’t really discuss the kidney cancer/tumor issue at all but more of a update on my status meeting. At the end, he said he will recommend to the teams to move forwared with the transplant. My sister will have to repeat some tests that are over a year old, and I’ll need to do a heart stress test and get a colonoscopy. Crap!
After speaking to the medical director, my transplant coordinator came one the line. I don’t think I’ve talked to her before. She said the previous coordinator I spoke was mainly for people on hold. Since I’m active now, whe will be my coordinator. I feel a lot better that they’re not rejecting or delaying my sister as a donor. As long as we pass the medical tests, I think the transplant will come fairly soon.
==========
My coordinator just called me again asking if the doctor specifically mentioned the cancer risk if I accept my sister’s kidney. He did not go over that part even though it was the original purpose of the call. Sigh… he may have to call me back again. The neverending story…
UCLA transplant center sent me a FedEx envelope today. I knew it was coming; the coordinator assistant told me over the phone she would send it out Monday. In it are instructions for this Friday’s video call, and another consent form. There is also other lists I need to fill out for medication and current physicians. The new item seems to be a consent for blood type B patients to receive kidney from blood type A2/A2B donors. The documentation said the risk of rejection is similar to a regular type B kidney. Of course I’ll take it. There is also consent forms to receive Hepatitis C or HIV infected kidneys but I was told to ignore those for now.
I believe these are standard forms for a new kidney patient. It’s kind of weird that I’ve filled these out three or four times already. Each time my donor is being reevaluated, they send out the forms. However, the main reason that this call is set up was them to explain the situation with my sister as donor. I guess I’m cautiously optimistic that they’re moving forward with the process again but not looking forward to retesting again at UCLA. At least the traffic is better now with COVID-19.
Actually, I have no idea what to do with the documents after I fill them out. Send back via FedEx? Scan to PDF and email? Is that allowed under HIPAA? I guess I’d better call the coordinator assistant tomorrow.